







Cerec
What is cerec?

CEREC (Chairside Economical Restoration of Esthetic Ceramics, or CEramic REConstruction) is a CAD and CAM method developed by W. Mormann and M. Brandestini at the University of Zurich in 1980 for reconstructing tooth restorations. This time-saving, computer-aided process allows dentists themselves to efficiently construct, produce, and insert individual ceramic restorations directly at the point of treatment (chairside) in a single appointment. The first applications were successfully carried out on patients in 1985.
General
In dentistry, the term CAD/CAM refers to the
digital workflow of a tooth restoration
treatment. This process entails making a digital
impression, constructing the restoration on the
computer (computer-aided design), and
manufacturing the restoration (computer-aided
manufacturing). In order to carry all of these
steps out in the dentist s office chairside the
dentist requires an imaging unit with an
intraoral camera, the corresponding construction
software, and a milling machine. If the dentist
is not looking to carrying out the entire
treatment process at the office, they do not
need a milling unit, but can instead send the
CAD/CAM data to the dental laboratory via an
online portal. The lab takes over the next few
steps and then sends the finished restoration
back to the dentist s office. Around 38,000
dentists worldwide use the CEREC method and thus
produce some 6.9 million restorations each year
(as of October 2013).
Model History
The CEREC method was developed by Prof. Werner
H. Mormann and Dr. Marco Brandestini at the
University of Zurich in 1980. The first patient
was treated with CEREC using VITABLOCS Mark I
ceramic blocks in 1985. Siemens obtained the
license to market and further develop the CEREC
method in 1986 and launched the world s first
CAD/CAM system in dentistry in the form of CEREC
1 in 1987. The areas of indication of the CEREC
2 system introduced in 1994 comprised inlays,
onlays, crowns, and veneers. In 1997, the sale
of Siemens AG s dental division resulted in the
company Sirona. The Windows-based CEREC 3 system
was introduced in 2000. While these first three
models were based on 2D technology, 3D software
introduced in 2003 allowed dentists to construct
restorations based on virtual three-dimensional
models using the computer. While for some time
it was only possible to attach all-ceramic
crowns adhesively, the increased precision of
the new generation of milling machine, MC XL,
which was launched in 2007, made it possible to
attach crowns using dental cement. In 2009,
Sirona switched to a new imaging technology, the
CEREC Bluecam, which is based on short-wave blue
light, thus significantly increasing the level
of precision in comparison to the previous 3D
camera. Since 2010, the use of Biogeneric has
made it possible to individually reconstruct the
occlusal surfaces of damaged or missing teeth,
while achieving a natural look. An
interdisciplinary research group headed by Prof.
Dr. Albert Mehl of the University of Zurich and
Prof. Dr. Volker Blanz of the University of
Siegen discovered that all of a patient s teeth
have individual characteristics that can be
applied from one tooth to another. Launched in
2011, the 4.0 version of the software simplified
the user interface with intuitive menu
navigation. Since then, it has also been
possible to work on several restorations within
a single process (multiple restorations). The
latest development is the CEREC Omnicam
intraoral camera, which was launched on the
market in 2012 and facilitates powder-free
digital impressions in natural colors.

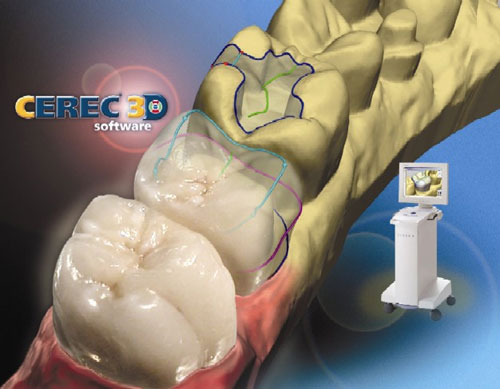
Technology
During a chairside treatment, the dentist
carries out all the steps, from digital
impressions and computer-based construction of
the restoration to the milling process, inside
their office. The dentist uses an intraoral
camera to take a photo of the preparation, the
antagonist teeth, and the bite situation. Based
on the images, the CEREC software creates a
virtual model of the patient s tooth situation.
The dentist uses this model to construct the
tooth restoration on the screen and then passes
on the finished construction within the office s
network or sends it wirelessly to a milling
machine. Depending on the type of restoration,
it is then milled out of a color-matched ceramic
block in just 6 to 15 minutes using
diamond-coated milling units. The dentist can
then add the finishing touches to the
restoration by painting, polishing, and glazing
it, before cementing it (the more traditional
option) or adhesively integrating it, depending
on the type of ceramic used.
Indications and materials
Silicate ceramics (feldspar and glass ceramics)
in particular are ideal for single tooth
restorations (inlays, onlays, crowns, and
veneers) in the front and on the sides of the
mouth. The comparably low flexural strength of
100 to 450 megapascals makes adhesive attachment
necessary. Lithium disilicate is a glass
ceramic, yet exhibits the material
characteristics of oxide ceramics. It is
exceptionally strong and translucent. Oxide
ceramics in particular are ideal for
manufacturing high-strength bridge frameworks
and crown copings in the front and on the sides
of the mouth. Flexural strength of 300 to 600
megapascals (infiltration ceramics) or 600 to
1,300 megapascals (polycrystalline oxide
ceramics) ensures a high level of long-lasting
durability and breaking strength.
Benefits
CEREC technology makes it possible to produce
and integrate ceramic restorations in a single
appointment. Unlike other materials such as
amalgam or gold, ceramic is more biocompatible
and boasts tooth-like physical and aesthetic
qualities. In addition, digital impressions are
more comfortable for patients than traditional
impressions.
By further developing the process, it was
possible to reduce the amount of follow-up work
and time-intensive occlusion adjustment that was
often necessary in the past. According to
studies, the ten-year lifespan of CEREC inlays
polished and milled with the aid of a computer
is not only significantly longer than that of
gold inlays, but also exceeds that of
individually laboratory-manufactured ceramic
inlays. Further clinical studies reveal that the
success rate of CEREC restorations is 95.5
percent following a period of nine years and 84
percent after 18 years.
Other potential applications
Combined with three-dimensional X-ray
technology, it has also been possible to use
CEREC for implants since 2009. The dentist can
combine the CAD/CAM planning based on CEREC with
3D X-ray data in order to coordinate the
prosthetic and surgical implant planning and
achieve the intended treatment results. Based on
this so called integrated implantology, the
dentist is able to order the drilling templates
from the drilling template manufacturer SiCat or
if they have their own milling machine produce
them on their own at the office using CEREC
Guide.